How to improve women's health in poor countries
It has long been established that women face many health problems largely because of their roles in society 1. However, some of these health problems are also due to the lack of provision of health services irrespective of gender 2. The scarcity of financial resources 3 and the lack of governmental commitment to address health problems 4 are two of the crucial factors that result in inadequate facilities and the lack of trained professionals in health services.
Everyday problems, like long waiting periods to see an obstetrician in emergency care, may seem like commonplace issues, but very often they are indirectly due to the poor management of the healthcare system 5 6. Health-related research could consider the broader picture by evaluating the role of authoritative figures in improving health care.
The focus on personal health problems that many women face in developing nations could be shifted on to policy makers. As such, I am going to discuss the role of the government in addressing maternal mortality, female genital mutilation (FGM), and cervical cancer. These are some of the most important public health concerns for women in low-income countries, and although there has been progress, local governments and international organisations should continue to address these issues in order to achieve health equity.
Maternal Mortality
Graph: World Economic Forum — How Much Has Maternal Health Improved?
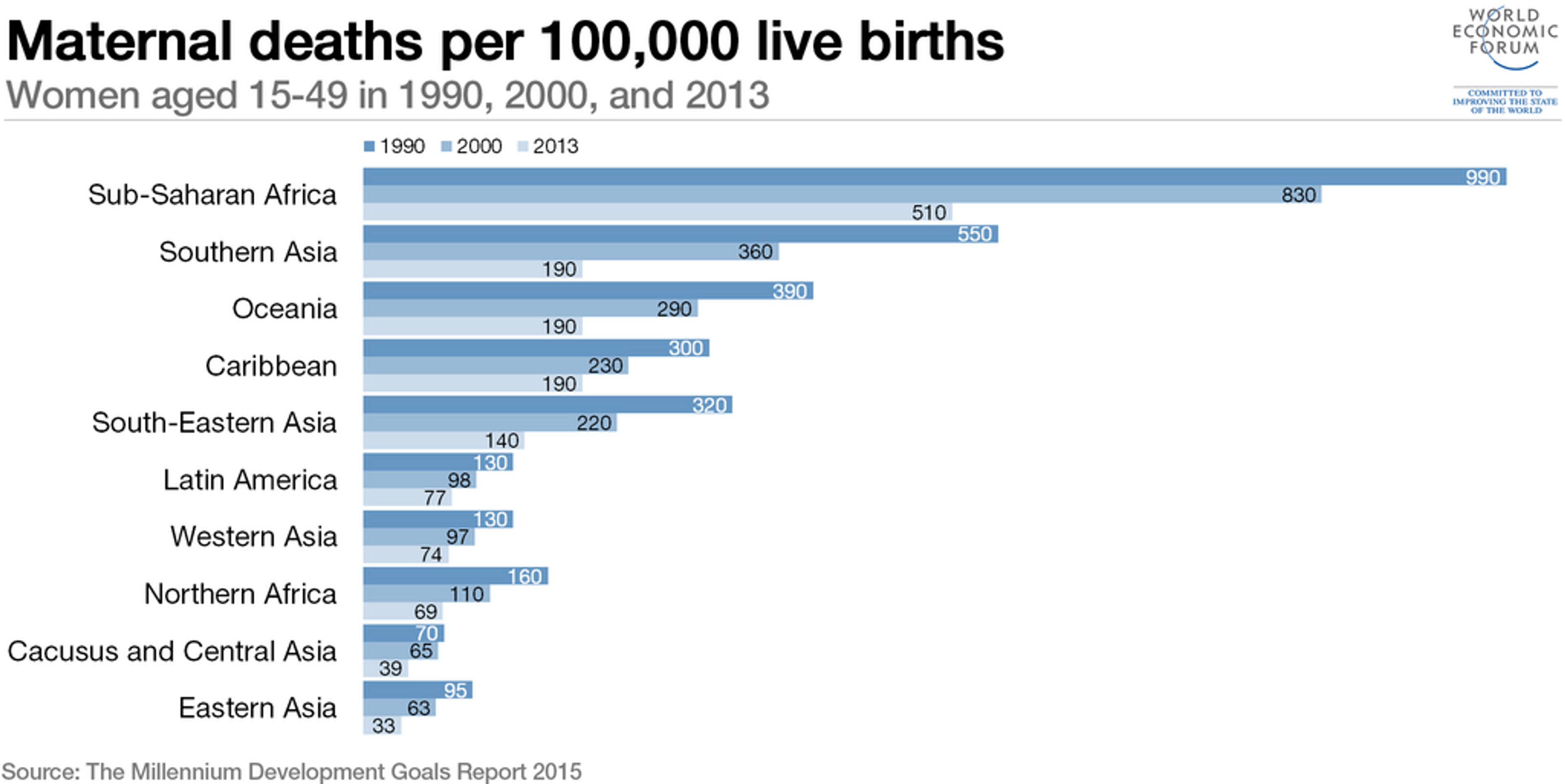
Some direct causes of maternal mortality include risks relating to pregnancy and childbirth as well as the poor quality of the health services 7. Other indirect causes, such as malaria 8 and anaemia from micronutrient deficiency 9 could also increase mortality rates. Though deaths due to malaria are hard to estimate and subject to substantial uncertainty, the World Health Organization (WHO) estimates that malaria accounted for the death of over 10,000 pregnant women in 2009 10.
Almost all of these deaths occur in developing countries 11, and many of them are preventable. Complications from pregnancy or childbirth are often associated with the lack of effective emergency obstetric care 11,12, and the lack of family planning programmes 12.
Pregnant women in developing nations, especially those living in rural areas, lack access to health services 13. There are few obstetric care facilities available, especially in rural parts of these countries. Other barriers include the inadequate quality of the facilities and the shortage of trained staff 13. Even if they are available, the cost of health care services might also prevent mothers from seeking help 13.
Two crucial factors to reduce maternal mortality are the availability of skilled professionals in delivery (e.g., midwives and obstetricians) and emergency obstetric services (e.g., Caesarean section) 14. This would require an effective health system which includes highly trained staff and well-equipped facilities. Unfortunately, most low-income countries spend less than necessary on health services, including emergency obstetric care 14.
It is important for governments to invest more in infrastructure to prevent maternal mortality. The use of maternal health services would be greater if policy makers were more involved in public spending on maternal health, and financing interventions such as skilled birth attendants and Caesarean section 14. The cost-effectiveness of providing cesarean delivery services can be as low as US$251 for each Disability adjusted life year averted in countries with high maternal morbidity risk15.
Direct out-of-pocket payments also deter people from utilising health services 14, and this can lead to pregnant women using untrained professionals for delivery and antenatal care, which could result in complications. It is estimated that approximately 16-33% of maternal deaths could be avoided by skilled attendants during delivery 16. These people are trained to address the four main complications commonly experienced in developing nations (obstructed labour, eclampsia, puerperal sepsis, and obstetric haemorrhage) 16, and unskilled attendants are often unable to deal with such issues, which results in death.
The case of Sri Lanka is evidence that long-term government commitment to improving health services for pregnant women can successfully reduce mortality rates in low-income countries 17. Between 2005-2015, maternal mortality rates have been steadily decreasing at the annual rate of 3.4% 18. The maternal mortality ratio has declined from 75 per 100,000 live births in 1990 to 30 per 100,000 live births 2015 18. This is a huge improvement. Policies were implemented to improve maternal health services by expanding the antenatal care services, increasing the number of skilled attendants (e.g., midwives), and introducing family planning programmes 17. Sri Lanka’s active malaria eradication campaigns could also have reduced maternal mortality rates [18-21] as malaria in pregnant women could lead to anaemia 19. Anaemia accounts for 8-16% of the direct causes of maternal deaths worldwide, and is a major contributor to side-effects such as infection, haemorrhage, and eclampsia, which could result in death 20.
Family planning programmes not only reduce the number of unplanned pregnancies, but also decrease the number of maternal deaths by reducing deaths associated with abortions in the case of unwanted pregnancies 21. It is estimated that contraceptives have reduced 44% of maternal deaths in the 172 countries analysed in 2008 22. Maternal mortality associated with unsafe abortion is the one that is most easily prevented. Hence, the provision of contraceptives and the access to safe abortions would reduce overall maternal mortality 21.
Government officials should invest in family planning programmes alongside maternal care, as evidence has shown greater efficacy than maternal care alone in reducing maternal mortality 23. Overall, the significant reduction in maternal mortality when skilled attendants, investment in emergency obstetric care, and education were implemented in Matlab, Bangladesh 24 shows that investment in these measures is crucial.
Female Genital Mutilation (FGM)
Female genital mutilation (FGM) is defined as “the partial or total removal of the female external genitalia or other injury to the female genital organs for non-medical reasons” 25. FGM has negative health consequences for those who have undergone the procedure, including, commonly, shock caused by pain or haemorrhage, infections, and pain when passing urine and faeces. Other long-term consequences include increased risk of complications during childbirth and increased risk for urinary tract infections (UTIs). Women who are subjected to FGM are also more likely to suffer from psychiatric disorders, such as depression and anxiety 26.
Currently, there are over 100 million girls under the age of 15 who are subjected to FGM 2728. In many African nations, FGM is ingrained in their cultures. Although the practice is less popular than before, action could still be taken to ensure that the practice of FGM is completely eradicated.
FGM was recently included in the new Sustainable Development Goals (SDGs) to “eliminate all harmful practices, such as child, early and forced marriages and female genital mutilations.” (Target 5.3). The WHO 25 has called for governments to establish legislative measures to protect girls from FGM, and promote awareness and public support to end the practice. Sadly, governments rarely prioritise FGM in their agenda.
The elimination of FGM requires the full commitment of government 29. Countries where FGM is prevalent should introduce stricter laws to prosecute adults (e.g., parents, community leaders) who allow girls to be subjected to FGM, and implement policies to raise the awareness of the harmful consequences of FGM at the same time. Medical practitioners who perform FGM on their clients should undergo disciplinary proceedings, and have their medical licenses revoked 30. An interagency statement (including UN Human Rights, UNICEF, and WHO) has urged governments to undertake these measures 30.
Governments should also liaise with community leaders, as illegal practices are prevalent despite the ban in some countries. It has been suggested that greater dissemination of information about FGM is crucial to improving practices 31. By garnering the support of community elders, awareness of the harmful consequences of FGM could be improved.
Cervical Cancer
Cervical cancer is the second most common cancer amongst women under the age of 35 in the world, and the most prevalent cancer in developing countries 1132. Most cases are linked to certain types of human papillomavirus (HPV), which are commonly passed on during sexual activity. As such, cervical cancer is preventable with regular HPV testing or HPV vaccines. These interventions can be highly cost-effective (we have written about this before).
Cervical cancer is a major public health concern (especially in sub-Saharan African countries), but unfortunately it is not given the priority that it deserves 33. Evidence showed that effective HPV screening programmes can promote early detection of cervical cancers 34.
Currently, in the UK, all girls aged between 12 and 13 years are offered HPV vaccination as part of the NHS childhood vaccination programme. However, due to the lack of financial resources, many developing countries are unable to introduce such programmes. Currently, only eight developing countries - Ghana, Kenya, Lao PDR, Madagascar, Malawi, Niger, Sierra Leone, and Tanzania - have received funding from GAVI to introduce pilot programmes 35.
Another cost-effective alternative would be to target HPV screening in high-risk women 34, and implement educational programmes at the same time. Educating people about cervical cancer is an effective preventative measure and promotes help-seeking behaviour at the same time 36. The WHO suggests that countries should implement the control of cervical cancer through establishing a national cancer control programme, and integrating cervical cancer into primary sexual and reproductive health services.
Alternatives to the expensive cytology-based screenings could include visual inspection of the cervix after application of 3-5% of acetic acid (VIA) as well as other VIA methods using magnification devices, visual inspection after the application of Lugol's iodine, or HPV DNA testing, all proposed alternatives to cervical cancer prevention screening tests 37.
Conclusion
These are merely some of the issues that many women face in developing nations. There are more deep-seated factors underlying these problems. For instance, the status of women (i.e., the political, educational, cultural roles they play in society) has a direct impact on their access to healthcare. Therefore, when we address these problems, we also need to consider the role of women as well as the cultural differences between various countries.
For example, many low-income countries are patriarchal societies where the ultimate decision lies in the hands of the men in the family, such as the husbands, fathers, or brothers (e.g., Ethiopia, Nigeria, India) 38. The perception of male superiority is also prevalent in many Asian societies, and people may be reluctant to pay for the cost of health services for women. Additionally, women who live in rural areas also do not often have driving licenses or do not own motorised vehicles, which would impede their access to health care services, especially those with specialised care facilities 38.
Hence it is crucial to push for women empowerment around the globe. Health organisations should liaise with organisations such as UN Women to educate people on the importance of women's rights, including their rights to health services.
Government officials have an important role to play. The lack of political support thus far has contributed to the slow progress. By advocating for political figures to be more involved in women’s health, effective altruists can have a more far-reaching impact on improving the lives of women in developing nations. For instance, effective altruists can conduct more research on effective ways to encourage governments to implement the measures mentioned above. Those who are interested in policy-making can collaborate with others to conduct cost-effectiveness analyses on various implementations that can improve the health systems.
They can also play a part in advocacy, by urging for government officials to commit to reduce maternal mortality rates, FGM cases and the prevalence of cervical cancer. By donating to NGOs, these organisations are not only pressuring the governments in developing nations to invest more in health, but also making a statement by highlighting the importance of addressing these issues. In fact, official development assistance for health to NGOs has significantly increased government health spending across the various developing countries 39. Public health issues are undoubtedly political. It is time for us as effective altruists to urge the governments to fully commit to these health problems.
Information based on WHO guidelines:
Maternal Mortalityhttp://www.who.int/mediacentre/factsheets/fs348/en/
Female Genital Mutilation (FGM) http://www.who.int/mediacentre/factsheets/fs241/en/
Cervical Cancer https://www.afro.who.int/health-topics/cervical-cancer