This post continues our update on Project Healthy Children.
Vitamin A
Vitamin A deficiency is the leading cause of preventable blindness in children and increases the risk of disease and death from severe infections [108] . In the recent Lancet series on maternal and child undernutrition, deficiencies of vitamin A were estimated to be responsible for 600,000 deaths per year, and together with zinc deficiency, a combined 9.8% of global childhood Disability-Adjusted Life Years (DALYs) (most deaths were due to diarrhea and measles: see Figure 16 ) [109] , [110] . Given that PHC’s work in Burundi has led to the start of vegetable oil fortification with vitamin A [111] , below we review the evidence for the cost-effectiveness of vitamin A fortification programmes.
Vitamin A fortification has been shown to be very cost-effective. A recent study from Uganda showed that the cost-per-DALY-averted for vitamin A fortification is only US $82 for sugar fortification and $18 for oil fortification [112] . A recent study suggested that even during prolonged deep frying with cooking oil, 45% of the fortified vitamin A remains intact, which is sufficient to meet daily requirements [113] . In line with this, a recent correlational study finds that it is strongly plausible that oil fortified with vitamin A increases vitamin A status in Indonesian women and children [114] .
Givewell has extensively reviewed Vitamin supplementation interventions [115] among them a large-scale trial [116] that found no reduction of mortality. This trial has led some researchers to suggest that Vitamin A policies should be revised, and that there should be more of an emphasis on vitamin A fortification as opposed to (biannual) vitamin A supplementation [117] . Other researchers have pointed to some severe limitations of the large trial and suggest that abandonment of vitamin A supplementation programmes is not prudent [118] . Moreover, an accompanying meta-analysis [119] suggested that taking into account all available evidence—including the large trial—simply yields a smaller estimate of 11% mortality reduction (rather than 25% as previously assumed). Benefits of vitamin A fortification are well established in western countries [120] and a Cochrane review to examine the effects of staple food fortification with vitamin A for preventing vitamin A deficiency is currently being conducted [121] .
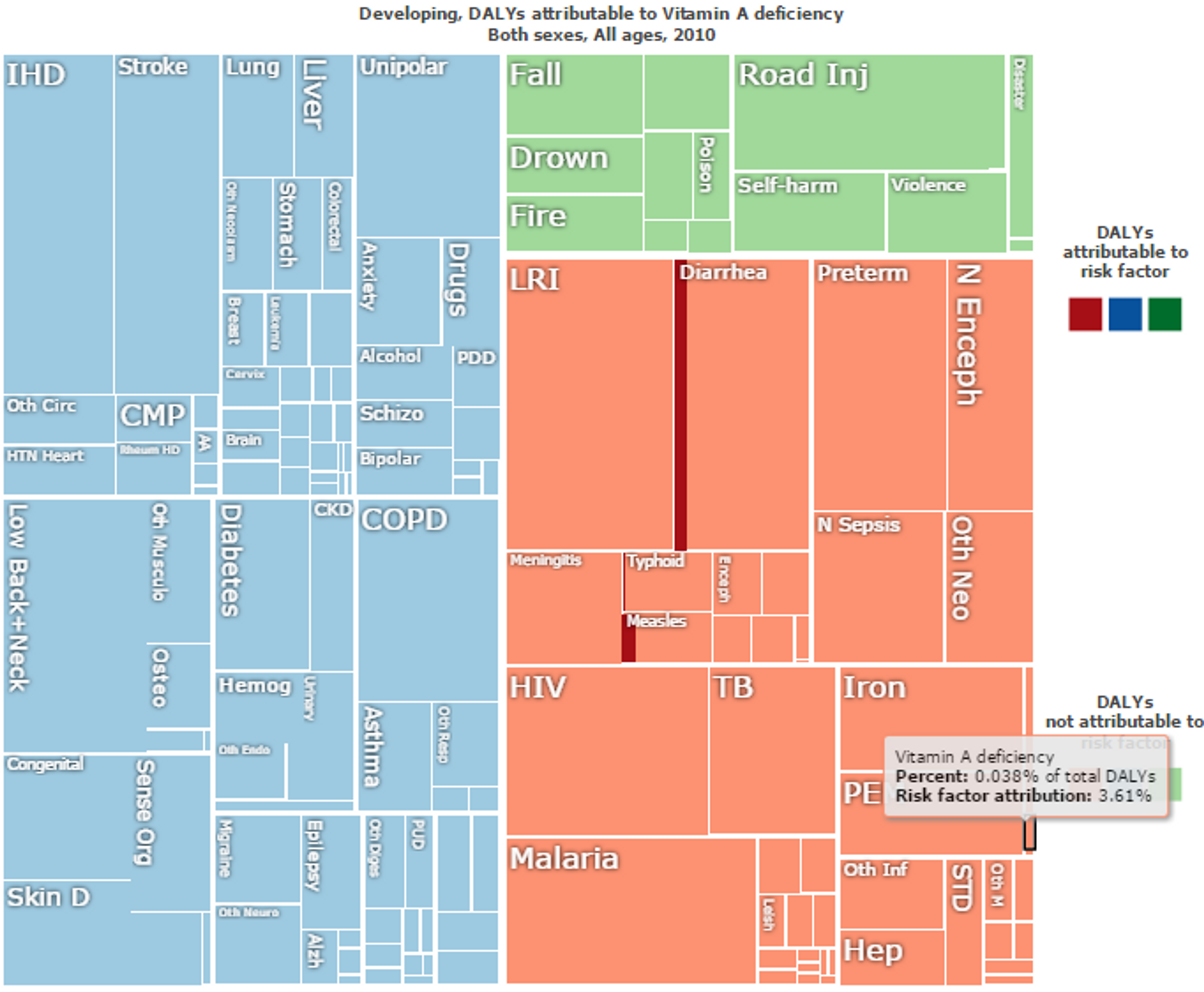
Figure 16: Overall “Disability Adjusted Life Years (DALYs)” lost in developing countries. Vitamin A deficiency direct impact is marked in black and make up 0.038% of the total DALYs. Risk factor attributions of Vitamin A deficiency for other diseases are in red. For instance, Vitamin A deficiency accounts for 10% of the risk factor of DALYs lost to do Diarrhea and 15% of DALYs lost due to Measles. Figure adapted with ‘Global Burden of Disease Compare tool’- see http://ihmeuw.org/3ba4 © 2013 University of Washington ** -** **Institute for Health Metrics and Evaluation **(Global burden of Disease data 2010, released 3/2013)
Vitamin A deficiency - disease interactions and risk factors
Vitamin A deficiency interacts with other conditions, increasing the risk of contracting other diseases. For instance, DNA damage from micronutrient deficiencies is likely to be a major cause of cancer [122] and a recent meta analysis clearly demonstrated that low doses of vitamins can significantly reduce the risk of gastric cancer, especially vitamin A among other vitamins [123] .
Vitamin A deficiency is also associated with hepatitis C infection and not being responsive to antiviral therapy [124] .
Research also suggests that vitamin A supplementation is beneficial for thyroid function and size—and potentially more so in combination with iodized salt [125] .
Studies have also linked vitamin A deficiency to infection with certain types of worm infections (i.e., soil-transmitted helminth Ascaris lumbricoides ), with robust evidence for a relationship between high-intensity ascaris infection and lower levels of vitamin A [126] .
Zinc
Zinc deficiency is a significant public health problem in developing countries [127] . In the recent Lancet series on maternal and child undernutrition, deficiencies of vitamin A and zinc were estimated to be responsible for 500,000 deaths per year, respectively, and together with zinc deficiency, a combined 9.8% of global childhood Disability-Adjusted Life Years (DALYs) [128] .
Zinc supplementation to children is cost-effective with one recent study estimating the cost per DALY averted at US$ 606 for pill supplementation, US$ 1,211 for micronutrient biscuits, and US$ 879 per DALY saved for water filtration systems [129] .
A recent trial from China [130] showed that zinc-fortified flour increases zinc levels in rural Chinese women. A Cochrane Review summarizing the evidence on fortification of staple foods with zinc for improving zinc status and other health outcomes in the general population is currently underway [131] . Finally, a recent trial showed that zinc supplementation might lead to a significant reduction in respiratory morbidity among children with acute lower respiratory infections in zinc-poor population [132] .
Folic Acid
Neural tube defects affect an estimated 320 000 newborns worldwide annually [133]
A systematic review Cochrane review concludes that folic acid supplementation, alone or in combination with vitamins and minerals, prevents neural tube defects [134] .
A recent trial from China [135] showed that folic acid fortified flour increases folic acid levels in rural chinese women.
A recent systematic review [136] on the on the Impact of folic acid fortification of flour on neural tube defects concludes that this intervention had a major impact on neural tube defects in all countries where this has been reported. For instance, the authors report that folic acid fortification in Chile showed a 55 % reduction in neural tube defect prevalence between 1999 and 2009 (this is a fairly typical effect: countries that mandate folic acid fortification of wheat flour report an average reduction of 46% in NTD birth prevalence [137] ). We found several studies that were not included in this review that show similar effects: after food fortification with folic acid is introduced, or folic acid intake is increased, folate levels increase and neural tube defects often decrease [138] , [139] , [140] , [141] .
Neural tube defects place a significant economic burden on the healthcare system and the wider society [142] and for this reason folic acid fortification also has a very good benefit cost ratio of 12–48:1, depending on the country [143] .
A recent meta-analysis and systematic review found no evidence that folic acid increase causes increase in bowel cancer [144] and another study found no increase in breast cancer or other cancers [145] .
Is biofortification more effective than industrial fortification?
Biofortification refers to the process of selectively breeding or genetically engineering crops to have higher micronutrient content. Even though this approach has not been practised so far, it has been suggested that it could potentially be more cost-effective and might reach a wider population than traditional industrial fortification of staple foods as conducted by PHC [146] , [147] . However, according to a recent paper by the Copenhagen Consensus Center [148] , in order to establish the cost-effectiveness of large scale biofortification, nutritional effectiveness must first be verified. In addition, acceptance of new plant varieties among farmers and consumers must be secured in order for biofortification to be a viable health intervention.
Updates on Room for additional funding
Long-term view on room for more funding
The data in Figure 17 suggest that, despite the potential for huge benefits, nutrition is grossly underfunded through aid [149] .
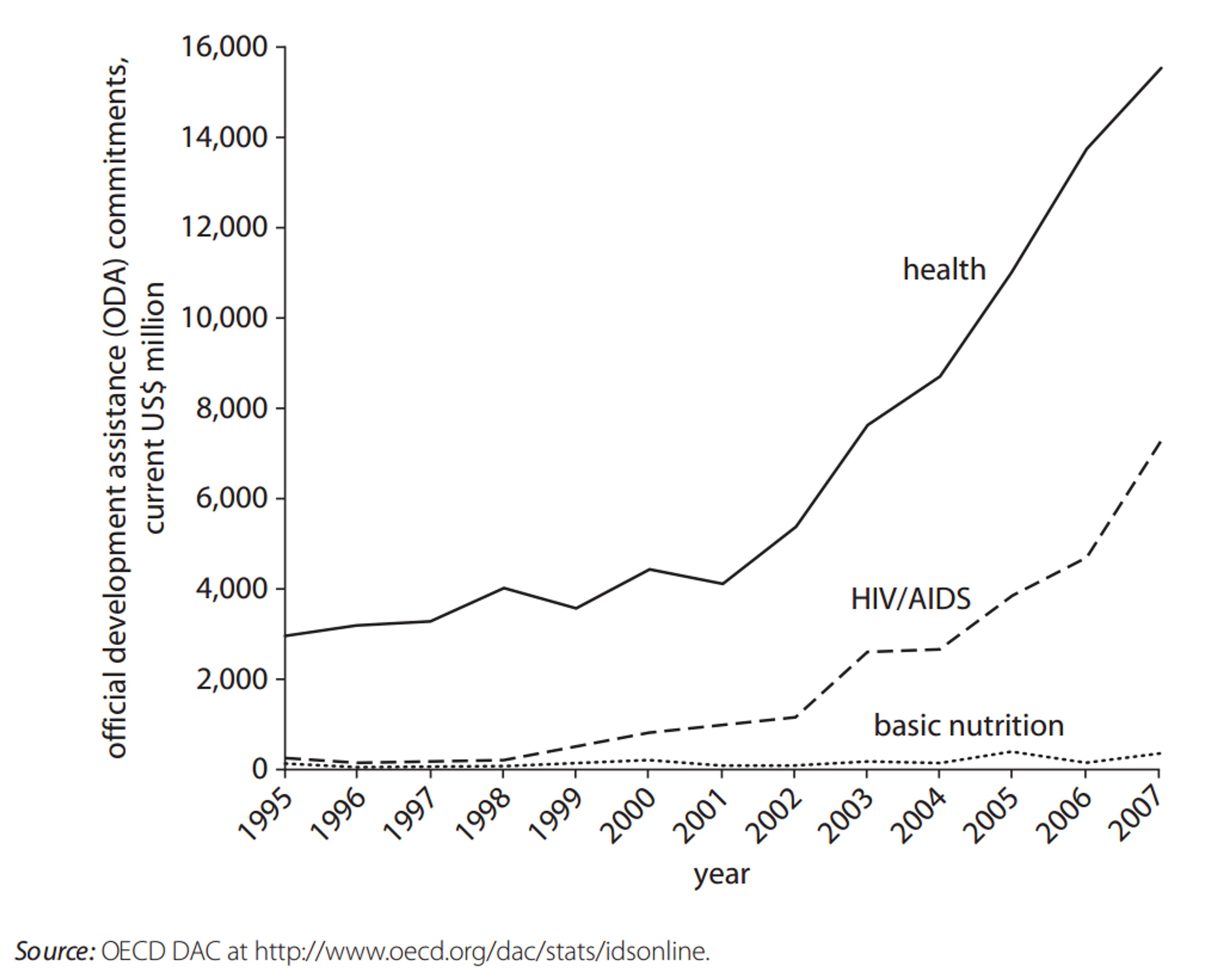
Figure 17 Official Development Assistance Commitments for Health, HIV/AIDS, and Nutrition, 1995–2007 [150]
Moreover, while aid for emergency food aid has increased dramatically (Figure 18), nutrition has remained chronically underfunded. [151]

Figure 18 Official Development Assistance Commitments for Nutrition and Emergency Food Aid, 1995–2007 [152]
Finally, as can be seen in Figure 19, nutritional deficiencies might be under researched, insofar as the number of studies published in the Cochrane database is fewer than would be expected given the global DALY and mortality burden of nutritional deficiencies.
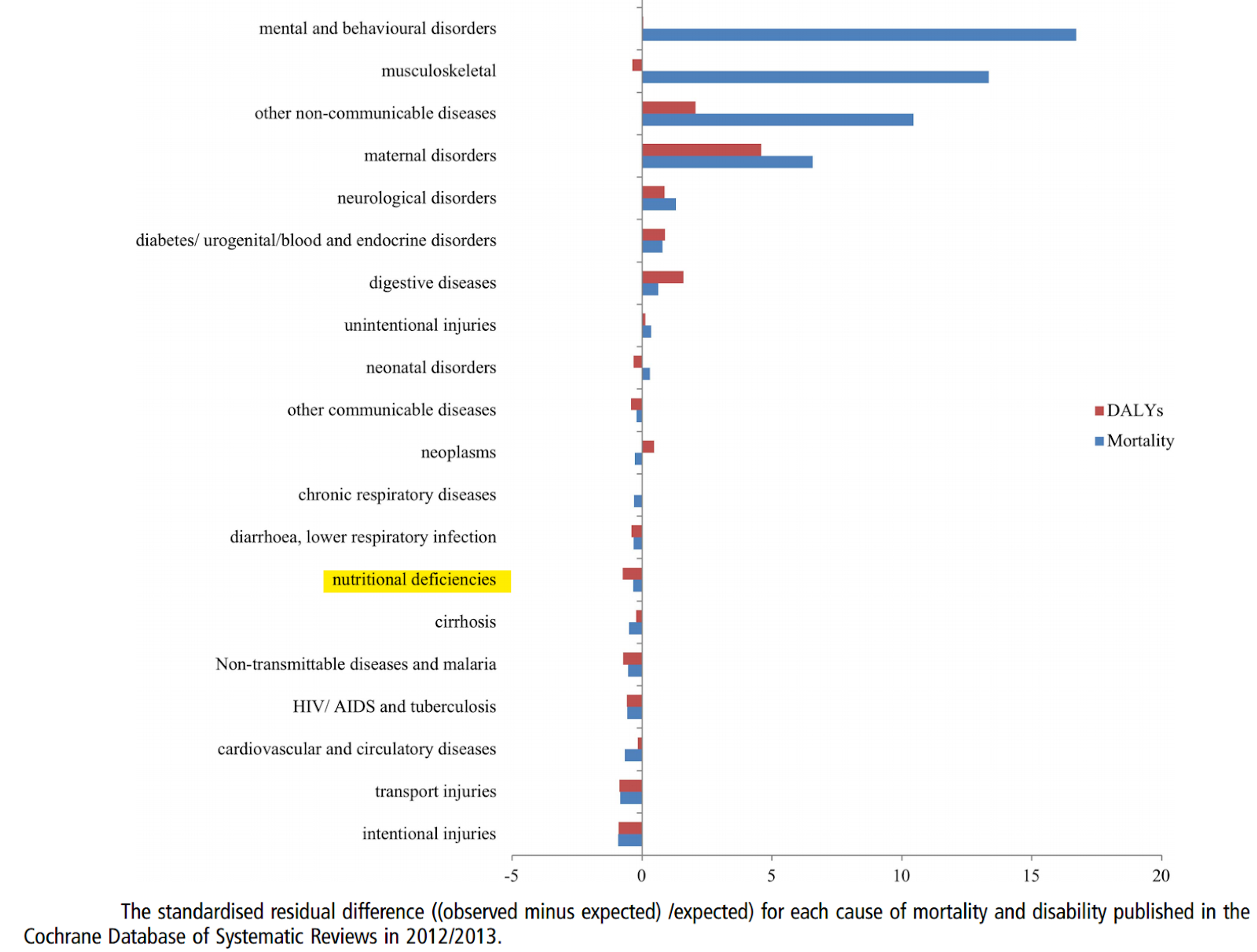
Figure 19: Nutritional Deficiencies are under researched in relation to their DALY and Mortality burden [153] .
How much more could be spend on nutrition? A recent review [154] suggests that the total annual cost of achieving 90% coverage in the the 34 countries most affected by nutritional deficiencies would be around $9.6 Billion (see Table 3 ).
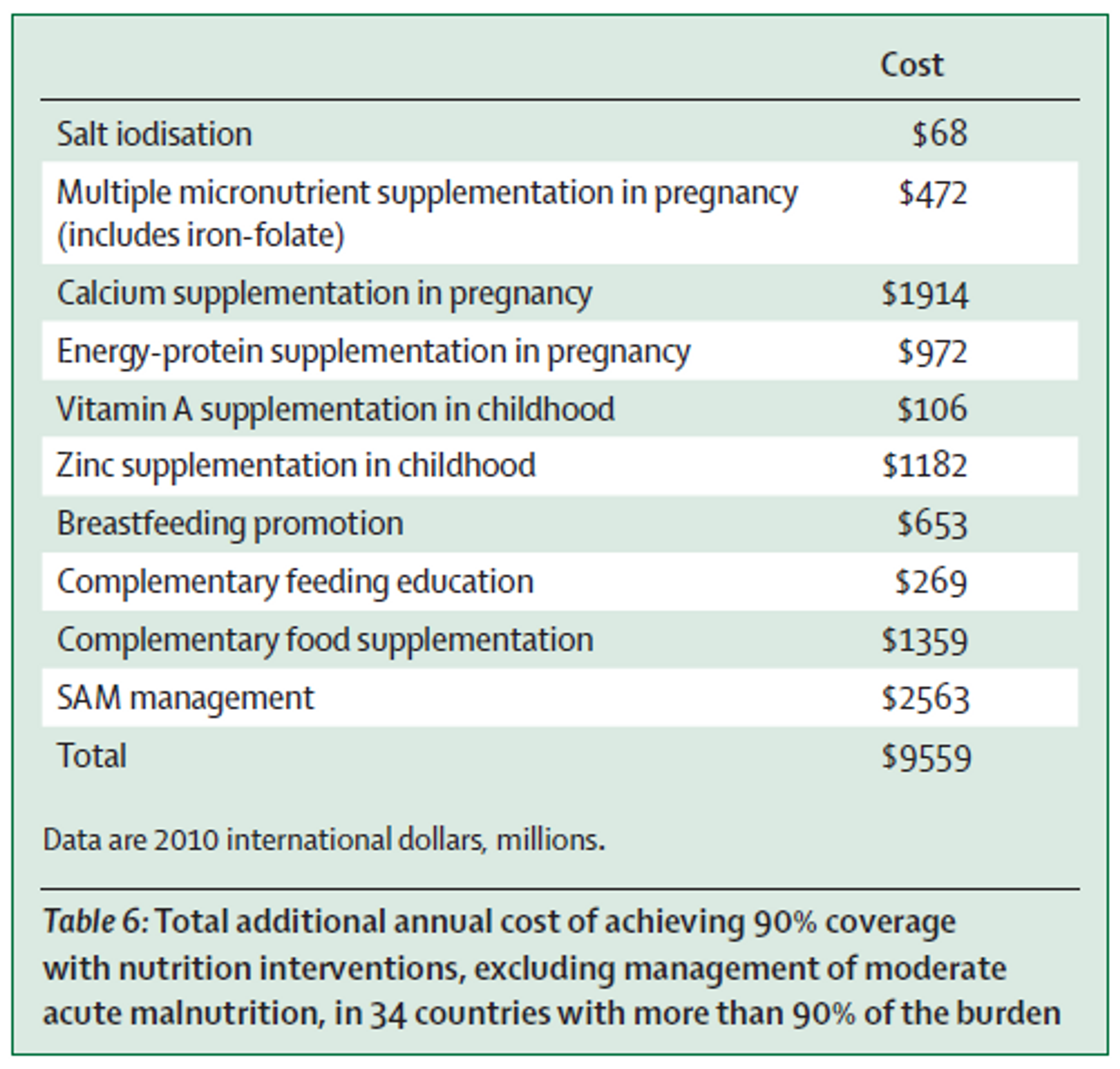
Table 3 : Total additional annual cost of achieving 90% coverage with nutrition interventions, excluding management of moderate acute malnutrition, in 34 countries with more than 90% of the burden.
This estimate is in line with a World Bank study [155] which estimated a funding gap of $10.3 billion per annum globally for scale-up of nutrition interventions. Closing this gap would provide preventive nutrition services to about 356 million children, save at least 1.1 million lives and 30 million DALYs, and reduce the number of stunted children by about 30 million worldwide. Another study by Bhutta et al. (2013) produced similar estimates.
Of course, not all of this money could be spent by PHC. However, we believe that PHC has substantial room for more funding, based on estimates of the cost required to implement micronutrient fortification in the countries where PHC is active. A recent World Bank report estimates that iron fortification of all staples in Sub-Saharan Africa would cost $130.5 million and salt iodization of all staples would cost $12.2 million per country. Although these costs would largely be paid for by the consumers of the fortified foods, there are substantial additional costs associated with full-scale implementation of fortification programs. Specifically, an additional US$50 million per year would be required for technical assistance, initial subsidy for fortificant, and social marketing for iron fortification and salt iodization; US$1.0 billion would be needed for capacity development for program delivery; and US$200 million for monitoring, evaluation, and operations research [156] . While these are projected worldwide costs, much of this investment would necessarily target Sub-Saharan Africa. Based on data from the World Bank, we estimate that the overall costs for scaling up micronutrient fortification programmes in countries where PHC is currently active (mostly small African countries), is around $33 million [157] .
A conversation in late 2012 between Givewell and a senior micronutrient adviser at UNICEF [158] , suggests that UNICEF does not have sufficient funding to meet every country’s need for Vitamin A supplementation. For instance, Uganda has solicited UNICEF and other donors for funding several times, indicating a strong need in Uganda for additional micronutrient funding, at least as of 2012. Other countries noted by the advisor as potentially having strong need for Vitamin A supplementation funding are Burundi, Comoros, Malawi and Rwanda. Project Healthy Children is currently active in all of these countries except for Comoros.
Other organisations involved in micronutrient fortification
We do not believe other organisations that are similar to PHC currently have as much room for additional funding as PHC. For instance, the Iodine Global Network (IGN) will receive approximately US $500,000 in funding from USAID in 2015 [159] and Global Alliance for Improved Nutrition (GAIN) has funding from the Bill and Melinda Gates Foundation through mid-2015, which may also be renewed [160] . Moreover, PHC is only active in small African countries with small populations (<17 million), whereas GAIN is not currently active in these countries [161] .
Gates Foundation’s recent investment in malnutrition
The Gates Foundation recently announced a $776 million investment in nutrition, which will also unlock matching funds from the United Kingdom. At least some of this money will fund food fortification [162] . However, the focus will be on India, Ethiopia, Nigeria, Bangladesh, and Burkina Faso [163] , and so it does not include any of the priority countries in which PHC currently works. This increases our confidence that the marginal dollar donated to PHC will not go to an already crowded funding landscape. At the same time, the fact that the Gates Foundation (which is very much concerned about cost-effectiveness and has vast research capacity and expertise) is investing in food fortification increases our confidence that food fortification should be a priority intervention.
Short-term view on room for more funding
PHC currently holds about $200,000 in reserves [164] , which translates to about 3-4 months of operational costs, which we think is not excessive. Thus, in the short-term there is room for more funding. PHC has told us that with additional funding they would intensify their monitoring efforts, which is one of the most critical components to any national fortification program.
Updates on Fundraising activities
PHC has told us that their current fundraising activities involve ‘news blasts’ and quarterly letters to current and previous donors. Yet it would seem that PHC has received less funding from private foundations and private donors than one might expect given the organization’s effectiveness, reputation, and room for additional funding. Therefore it may be a good idea for PHC to use additional resources to attract more funding (additional resources directed to non-program activities would not necessarily make Giving What We Can less likely to recommend donating to PHC; we assess charities based on overall effectiveness rather than exclusively on overhead costs). PHC is also now in the process of being evaluated by Givewell, which is a very good opportunity for them to receive increased exposure and funding.
Updates on PHC’s Operations
Fortification programs
Our colleagues at Givewell provide a great general overview of PHC’s operations in form of a conversation note with PHC’s Chief operating officer, Laura Rowe.
PHC reports its fortification program in Rwanda is almost completed and operations are being handed over to the local government. PHC’s efforts are now focused on industry engagement, consumer and policymaker awareness, and establishing an institutionalized monitoring and evaluation system [165] . They report that in 2015, priorities in Rwanda will be to (1) continue to support appropriate sourcing of equipment and premix; (2) secure gap funding where needed; (3) guide appropriate testing, monitoring, and reporting structures within industry and at the government level to track compliance; and (4) ensure the design of a surveillance system to track coverage and ultimately measure the impact of fortification on micronutrient status. Finally, PHC is working closely with the Rwandan Ministry of Health to secure funds for the hiring of a short-term Fortification Monitoring Specialist to be placed within the government to guide the program through this critical, post-implementation phase.
Similarly, in Sierra Leone, where PHC has been active since 2014, PHC reports that they are supporting the Ministry of Health in (1) drafting relevant fortification policies; (2) designing training protocols for inspectors of fortified foods; (3) creating advocacy structures; and (4) developing appropriate monitoring and reporting systems [166].
Acknowledgements
Thanks to the scientists who have given their expert opinion on different parts of this report.